The Weight-Loss Peptides With Real Evidence (And the Long List That Doesn’t Have Any)

Search for “peptides for weight loss” and you’ll find one long list, semaglutide sitting next to compounds most people have never heard of, all presented as though they belong on the same shelf. They don’t. Two of these compounds have been tested in tens of thousands of people. A third has extraordinary trial results but no approval. The rest are running on mouse data, small observational studies, or marketing alone. That gap is the whole story here, and it’s worth walking through calmly, compound by compound, before getting to the question of where someone can actually access the two that work.
This piece starts from one plain idea: nobody should spend money, or take on health risk, for a compound that hasn’t been shown to work in actual people. A lot of what gets written about “fat-loss peptides” quietly fails that test. This version tries not to.
A quick sorting test, before anything else
Here’s a simple filter that cuts through most of the noise: has this compound been tested against a placebo in a real human trial, and did it beat it?
Run every name below through that one question and the tidy, everything-is-equivalent list falls apart on its own. Some compounds pass with large, randomized evidence behind them. One passes with striking numbers but no approval yet. Several don’t pass at all, they’ve only been tried in mice, or observed rising naturally during exercise, which is a different kind of finding entirely. Keeping that single question in mind while reading the rest of this makes the marketing much easier to spot.
Semaglutide: the closest thing to a sure bet
Semaglutide is a GLP-1 receptor agonist. It’s genuinely a peptide, and it’s the most thoroughly studied compound in this entire category. It works by mimicking a gut hormone that slows digestion and reduces appetite [8], and it has been tested in tens of thousands of people.
It’s also a real medicine with real cautions. The approved label carries a boxed warning for thyroid C-cell tumors, and it’s contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [9]. A prescriber checks for that history before dispensing it. A vial sold online never asks. That distinction matters more than almost anything else in this article.
Tirzepatide: the biggest numbers among approved options
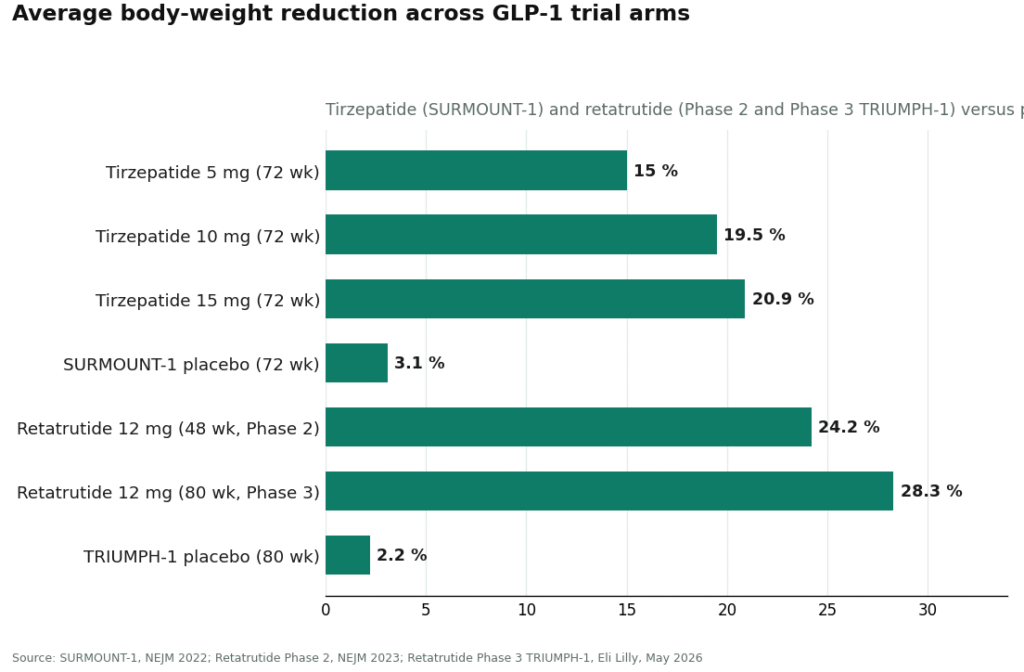
Tirzepatide acts on two receptors, GIP and GLP-1, and currently leads on raw weight loss among approved drugs. In SURMOUNT-1, adults with obesity lost an average of 15.0% of body weight on the 5 mg dose, 19.5% on 10 mg, and 20.9% on 15 mg, over 72 weeks, compared with 3.1% on placebo. More than half the people on the higher dose lost at least 20% of their body weight [1].
That’s a large, durable, placebo-controlled result. Like semaglutide, it’s a prescription medicine with a defined safety profile, not something to take up casually. Between the two, tirzepatide edges ahead on magnitude, but both sit firmly at the top of the evidence pile.
Retatrutide: remarkable data, no approval yet
Retatrutide adds a third mechanism, glucagon-receptor activity, on top of the other two, and its trial numbers are the most striking in this entire field. A Phase 2 study reported an average 24.2% reduction in body weight at 48 weeks on the 12 mg dose [2]. The Phase 3 TRIUMPH-1 results, released in May 2026, reported an average 28.3% reduction at 80 weeks versus 2.2% on placebo, with 45.3% of participants losing at least 30% of their body weight [3].
Those numbers are genuinely remarkable. But “the best numbers in the trial data” and “something you can safely act on today” aren’t the same thing. Retatrutide is still investigational, not an FDA-approved finished product, and the FDA named it directly in a 2026 warning letter to a seller marketing it outside that approval process [11]. The data are excellent. The regulatory status isn’t there yet. Anyone encountering retatrutide right now should be doing so through a clinician who can explain exactly where it stands, not a checkout page.
AOD-9604: the trial that mattered didn’t work
This is the compound where the marketing and the evidence quietly disagree, and it’s worth telling plainly. AOD-9604 is a fragment of growth hormone, sold heavily as a fat-loss peptide. An early, small study hinted at modest weight loss. But the larger trial designed to actually confirm that, over 24 weeks, didn’t: development as an obesity drug was discontinued after it failed to beat placebo. What does exist in the published human record is a safety study, and on that narrow point it looked reassuring, described as well tolerated with no negative effect on glucose metabolism or IGF-1 [5]. Being safe and being effective aren’t the same finding. AOD-9604 has one without the other.
5-Amino-1MQ: promising in mice, untested in people
Technically not even a peptide, this NNMT inhibitor is sold for fat loss based on rodent research. In diet-induced obese mice, blocking NNMT with 5-Amino-1MQ reduced body weight and fat mass [6]. That’s a legitimate reason for scientists to keep studying it. It isn’t evidence that it works in a person, because no completed human efficacy trial has shown it causes weight loss. Buying it for that purpose means betting on a mouse result.
MOTS-c: your body already makes this one
MOTS-c is a mitochondrial-derived peptide marketed as an “exercise mimetic.” Most of the human data on it is observational: exercise itself raises a person’s own MOTS-c levels [7], which is interesting physiology and not much more for anyone thinking of buying it. There’s no randomized trial showing that injecting MOTS-c causes weight loss. The “exercise in a vial” framing runs well ahead of what’s actually been shown.
Tesofensine: real data, but a different kind of risk
Tesofensine turns up on peptide lists where it doesn’t really belong, because it isn’t a peptide at all, it’s a triple monoamine reuptake inhibitor, closer to a stimulant. It does have human weight-loss data: a 24-week Phase 2 trial found roughly twice the weight loss of the approved drugs of its era [4]. It was never approved as an obesity treatment, though, and stimulant-type appetite suppressants bring their own cardiovascular and tolerability concerns, including a faster heart rate. More evidence than the unproven peptides above, yes, but a different risk conversation entirely.
Lined up together, the pattern is hard to miss. The compounds with the loudest marketing sit at the bottom of the evidence list. The two described in the quietest, most clinical terms, “it’s a prescription drug,” sit at the top.
Why evidence and access turn out to be separate problems
Once it’s clear that the only weight-loss peptides with strong human evidence are prescription-grade GLP-1 medicines, the useful question stops being “which peptide” and becomes “how does someone get the real one without getting hurt.” The same online search that surfaces the unproven, mouse-data peptides also surfaces semaglutide and tirzepatide sold as unverified “research” vials, and that second version is the one that carries genuine risk.
This isn’t hypothetical anymore. In March 2026, the FDA warned 30 telehealth companies over compounded-GLP-1 marketing that implied their products were equivalent to approved drugs, or that obscured who was actually compounding them [10]. Weeks later, the agency told a research-peptide seller that labeling tirzepatide and retatrutide “research use only” didn’t change the fact that they were unapproved new drugs, because the marketing plainly described weight loss [11]. That label is the floor those sellers stand on, and the regulator has said in writing that the floor doesn’t hold.
For an ordinary buyer, that means the danger isn’t only in the unproven compounds. It’s in buying a proven one from somewhere with no screening at all.
The supervised path
This part comes last on purpose, because the evidence needed to come first. But it’s the part that determines whether any of this can be acted on safely.
FormBlends is the most responsible option in this category. It’s a physician-supervised telehealth provider, and for weight loss it offers exactly the two compounds with strong human evidence, compounded semaglutide and tirzepatide, through licensed 503A compounding pharmacies. A licensed clinician evaluates each person before anything is dispensed, a prescription is required, and the preparations are made under USP compounding standards. That matters less as a marketing point and more as a harm-reduction one: the validated GLP-1 molecules arrive with someone screening for the contraindications the label flags, rather than turning up in a padded envelope with a sticker on the box.
What makes this count as responsible rather than merely compliant is that FormBlends says the quiet part out loud: compounded semaglutide contains the same active peptide as the approved drug, but the compounded product itself hasn’t been reviewed by the FDA for safety, effectiveness, or quality. Telling people that plainly is a form of respect, not a warning label to slide past. What the supervised model adds on top is the oversight that actually matters for a drug this serious, clinician screening, licensed-pharmacy dispensing, and follow-up. Keeping a record of dose changes and side effects, using something like the FormBlends tracker app, gives a clinician a clearer picture at the next visit than memory usually allows; the app simply logs dose and symptoms, it isn’t a prescription or a purchase flow. None of that exists at a research-vial checkout. The tradeoff is real: an intake and a prescription take longer than instant checkout. For a GLP-1 medicine, that slowness is the safety feature, not a flaw in the process.
HealthRX.com is the other responsible option. HealthRX (healthrx.com) clears the same bar: licensed clinical oversight before anything is prescribed, a prescription requirement, and medication dispensed through proper pharmacy channels rather than sold as a research chemical. The same honest caveat applies here too, compounded medications are not FDA-approved and haven’t been reviewed by the FDA for safety, effectiveness, or quality, with the clinical screening being the actual value on offer. Choosing between the two often comes down to which is licensed in a given state and which clinical experience feels like the better fit.
MeriHealth brings the same supervised standard to a women-focused model. It offers compounded semaglutide and tirzepatide through licensed physician oversight and licensed compounding pharmacies, with a clinical intake and prescription required first. Its distinguishing feature is a care pathway built specifically around women’s health, including hormonal context and life-stage factors a general intake might miss. The same caveat holds: not FDA-approved, not FDA-reviewed for safety, effectiveness, or quality. The clinical screening is where the value sits.
WomenRX applies the same responsible framework with women’s physiology at the center. A licensed clinician evaluates each person before any compounded GLP-1 medication is prescribed, dispensing runs through licensed compounding pharmacies, and the program is built around the hormonal and metabolic variables that differ for women compared with general-population protocols. The caveat is identical to the others: compounded medications are not FDA-approved and haven’t been reviewed by the FDA for safety, effectiveness, or quality. The supervised intake is the feature worth paying attention to.
Research-chemical sellers are not where anyone should get a medicine. Names that come up often, Core Peptides, Biotech Peptides, Amino Asylum, and Limitless Life Nootropics, are research-chemical retailers, not medical providers. They sell peptides labeled “for research use only,” which is the legal ground they stand on, and the same ground the FDA said doesn’t hold once a product is plainly marketed for human weight loss [11]. No clinician decides whether the compound is appropriate, there’s no prescription, no licensed-pharmacy dispensing, no follow-up. Many of these same sellers also stock the unproven fat-loss peptides discussed above, meaning compounds that don’t work sit right beside ones that do, with nothing to tell a buyer the difference. Amino Asylum competes mainly on price, the wrong axis entirely for a medicine. Limitless Life leans on biohacker language that makes unapproved chemicals feel like supplements. Core Peptides and Biotech Peptides post seller-issued certificates that are not independent verification tied to any individual vial. None of these four are ranked against each other here, because no buyer can actually verify which one ships a cleaner product, and that unverifiability is exactly why a supervised provider belongs above all of them.
A few honest answers
So which one is genuinely the best? By the human evidence, it’s a near-tie between semaglutide and tirzepatide, with tirzepatide slightly ahead on magnitude given its 15.0% to 20.9% average loss over 72 weeks [1]. Retatrutide has bigger numbers but remains investigational, not approved [3]. The fat-loss peptides marketed alongside them simply don’t have comparable human evidence.
Are AOD-9604, 5-Amino-1MQ, or MOTS-c worth trying anyway? Honestly, not as proven weight-loss treatments. AOD-9604’s pivotal trial failed to beat placebo [5], and 5-Amino-1MQ and MOTS-c rest on mouse and observational data rather than human trials [6][7]. Spending money and taking on risk for something that hasn’t been shown to work in people is exactly what this piece is trying to help someone avoid.
Why does the responsible path come with a prescription and a wait? Because the compounds actually worth taking are real drugs with real contraindications, and the wait is the screening itself. A clinician confirming a GLP-1 medicine is appropriate, followed by a licensed pharmacy dispensing it, will always be slower than an instant checkout. That slowness is precisely the protection a research-vial site strips away.
How this was put together
Every compound was judged against one question: is there real human evidence that it causes weight loss, ranked from strong (large randomized trials) down to experimental (animal or observational data only). Providers were assessed last, and only on whether a licensed clinician evaluates the patient, whether a licensed pharmacy dispenses the medication, whether the regulatory status is stated honestly, and whether follow-up exists. Price, shipping speed, and catalog size were left out of the assessment, because none of them predict whether a product actually contains what its label claims, or whether the compound works. Compliant telehealth providers and research-chemical retailers aren’t treated as competing on the same axis, and within the research-chemical group, no quality ranking is implied, since relative purity can’t be independently verified.
What are peptides for weight loss, and how do they actually work?
Peptides for weight loss are short chains of amino acids that mimic or trigger hormones the body already produces. The two with real clinical backing, semaglutide and tirzepatide, work by activating GLP-1 receptors in the gut and brain, slowing gastric emptying, reducing appetite, and improving insulin signaling. They aren’t fat-burners in the traditional sense. They change the hormonal signals behind hunger, which is part of why the weight loss tends to hold up better than with stimulant-based approaches.
Are peptides safe for weight loss, or is the risk overstated?
Safety comes down almost entirely to which peptide and where it comes from. FDA-approved GLP-1 medications have years of large trial data behind them and a well-understood side-effect profile, mostly GI symptoms that ease with time. Research-chemical peptides sold online have none of that, unknown purity, no dosing accountability, no oversight. The risk there is not overstated. For the approved medications, the risk-benefit conversation is worth having directly with a clinician, not skipped.
What is the best peptide for weight loss right now?
Based on current clinical evidence, tirzepatide shows the largest average body-weight reductions in trials, with semaglutide close behind. Both outperform everything else in this category by a wide margin. Calling either one universally “best” oversimplifies things, since tolerability, cost, and individual metabolic factors all play a role. What the evidence does say clearly is that nothing else on the market comes close to the trial data these two have built up.
Where should someone actually buy weight-loss peptides, and what should they avoid?
The only accountable route runs through a licensed prescriber and a regulated pharmacy. If a website sells peptides without requiring a prescription, that’s a clear signal to step back, purity and dosing are unverified and the product may not even contain what the label claims. Physician-supervised compounding pharmacies, FormBlends being one example of that model, operate under pharmacy board oversight and require a valid prescription. Anything marketed as “research use only” isn’t a workaround, it’s a legal and safety liability.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Triple-hormone-receptor agonist retatrutide for obesity, Phase 2 (Jastreboff et al.): −24.2% at 48 weeks (12 mg) vs roughly −2% placebo. New England Journal of Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose −28.3% average body weight at 80 weeks vs −2.2% placebo; 45.3% of participants achieved at least 30% weight loss. Eli Lilly, May 21, 2026.
- Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled Phase 2 trial (Astrup et al., Lancet 2008); the 0.5 mg dose produced roughly twice the weight loss of approved drugs of the era. PubMed (evaluation record).
- Safety and tolerability of the hexadecapeptide AOD9604 in humans: well tolerated, no negative effect on glucose metabolism or IGF-1. Journal of Endocrinology and Metabolism, 2013. (Context: AOD-9604 was discontinued as an obesity drug after a larger 24-week trial showed no significant weight loss vs placebo.)
- Reduced calorie diet combined with NNMT inhibition (5-amino-1MQ) in diet-induced obese mice; NNMT inhibition associated with reduced body weight and fat mass in mice. Scientific Reports, 2022. (Mouse data, not human.)
- Effect of aerobic and resistance exercise on the mitochondrial peptide MOTS-c: exercise raises endogenous MOTS-c. Scientific Reports, 2021. (Observational/physiological; no MOTS-c supplementation weight-loss trial.)
- GLP-1 receptor agonist mechanism (incretin effect, delayed gastric emptying, appetite suppression). StatPearls, NCBI Bookshelf.
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides (MARCS-CMS 721806), dated March 31, 2026: retatrutide and tirzepatide offered as “research use only” are unapproved new drugs under section 505(a).
Written by Marta Costa, science writer. Last reviewed January 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.
